Nov 21 JDN 459540
Most medical residents work 60 or more hours per week, and nearly 20% work 80 or more hours. 66% of medical residents report sleeping 6 hours or less each night, and 20% report sleeping 5 hours or less.
It’s not as if sleep deprivation is a minor thing: Worldwide, across all jobs, nearly 750,000 deaths annually are attributable to long working hours, most of these due to sleep deprivation.
By some estimates, medical errors account for as many as 250,000 deaths per year in the US alone. Even the most conservative estimates say that at least 25,000 deaths per year in the US are attributable to medical errors. It seems quite likely that long working hours increase the rate of dangerous errors (though it has been difficult to determine precisely how much).
Indeed, the more we study stress and sleep deprivation, the more we learn how incredibly damaging they are to health and well-being. Yet we seem to have set up a system almost intentionally designed to maximize the stress and sleep deprivation of our medical professionals. Some of them simply burn out and leave the profession (about 18% of surgical residents quit); surely an even larger number of people never enter medicine in the first place because they know they would burn out.
Even once a doctor makes it through residency and has learned to cope with absurd hours, this most likely distorts their whole attitude toward stress and sleep deprivation. They are likely to not consider them “real problems”, because they were able to “tough it out”—and they are likely to assume that their patients can do the same. One of the primary functions of a doctor is to reduce pain and suffering, and by putting doctors through unnecessary pain and suffering as part of their training, we are teaching them that pain and suffering aren’t really so bad and you should just grin and bear it.
We are also systematically selecting against doctors who have disabilities that would make it difficult to work these double-time hours—which means that the doctors who are most likely to sympathize with disabled patients are being systematically excluded from the profession.
There have been some attempts to regulate the working hours of residents, but they have generally not been effective. I think this is for three reasons:
1. They weren’t actually trying hard enough. A cap of 80 hours per week is still 40 hours too high, and looks to me like you are trying to get better PR without fixing the actual problem.
2. Their enforcement mechanisms left too much opportunity to cheat the system, and in fact most medical residents simply became pressured to continue over-working and under-report their hours.
3. They don’t seem to have considered how to effect the transition in a way that won’t reduce the total number of resident-hours, and so residents got less training and hospitals were less served.
The solution to problem 1 is obvious: The cap needs to be lower. Much lower.
The solution to problem 2 is trickier: What sort of enforcement mechanism would prevent hospitals from gaming the system?
I believe the answer is very steep overtime pay requirements, coupled with regular and intensive auditing. Every hour a medical resident goes over their cap, they should have to be paid triple time. Audits should be performed frequently, randomly and without notice. And if a hospital is caught falsifying their records, they should be required to pay all missing hours to all medical residents at quintuple time. And Medicare and Medicaid should not be allowed to reimburse these additional payments—they must come directly out of the hospital’s budget.
Under the current system, the “punishment” is usually a threat of losing accreditation, which is too extreme and too harmful to the residents. Precisely because this is such a drastic measure, it almost never happens. The punishment needs to be small enough that we will actually enforce it; and it needs to hurt the hospital, not the residents—overtime pay would do precisely that.
That brings me to problem 3: How can we ensure that we don’t reduce the total number of resident-hours?
This is important for two reasons: Each resident needs a certain number of hours of training to become a skilled doctor, and residents provide a significant proportion of hospital services. Of the roughly 1 million doctors in the US, about 140,000 are medical residents.
The answer is threefold:
1. Increase the number of residency slots (we have a global doctor shortage anyway).
2. Extend the duration of residency so that each resident gets the same number of total work hours.
3. Gradually phase in so that neither increase needs to be too fast.
Currently a typical residency is about 4 years. 4 years of 80-hour weeks is equivalent to 8 years of 40-hour weeks. The goal is for each resident to get 320 hour-years of training.
With 140,000 current residents averaging 4 years, a typical cohort is about 35,000. So the goal is to each year have at least (35,000 residents per cohort)(4 cohorts)(80 hours per week) = 11 million resident-hours per week.
In cohort 1, we reduce the cap to 70 hours, and increase the number of accepted residents to 40,000. Residents in cohort 1 will continue their residency for 4 years, 7 months. This gives each one 321 hour-years of training.
In cohort 2, we reduce the cap to 60 hours, and increase the number of accepted residents to 46,000.
Residents in cohort 2 will continue their residency for 5 years, 4 months. This gives each one 320 hour-years of training.
In cohort 3, we reduce the cap to 55 hours, and increase the number of accepted residents to 50,000.
Residents in cohort 3 will continue their residency for 6 years. This gives each one 330 hour-years of training.
In cohort 4, we reduce the cap to 50 hours, and increase the number of accepted residents to 56,000. Residents in cohort 4 will continue their residency for 6 years, 6 months. This gives each one 325 hour-years of training.
In cohort 5, we reduce the cap to 45 hours, and increase the number of accepted residents to 60,000. Residents in cohort 5 will continue their residency for 7 years, 2 months. This gives each one 322 hour-years of training.
In cohort 6, we reduce the cap to 40 hours, and increase the number of accepted residents to 65,000. Residents in cohort 6 will continue their residency for 8 years. This gives each one 320 hour-years of training.
In cohort 7, we keep the cap to 40 hours, and increase the number of accepted residents to 70,000. This is now the new standard, with 8-year residencies with 40 hour weeks.
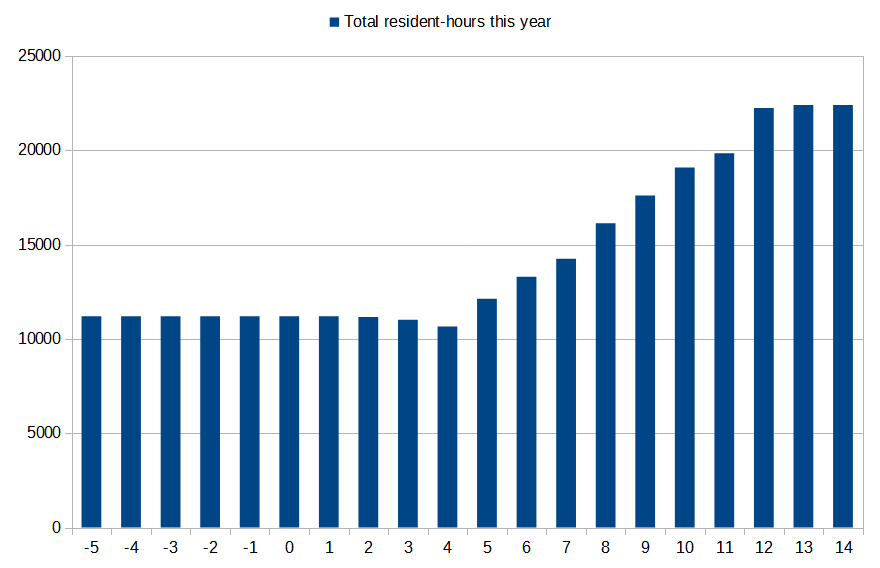
I’ve made a graph here of what this does to the available number of resident-hours each year. There is a brief 5% dip in year 4, but by the time we reach year 14 we’ve actually doubled the total number of available resident-hours at any given time—without increasing the total amount of work each resident does, simply keeping them longer and working them less intensively each year. Given that quality of work is reduced by working longer hours, it’s likely that even this brief reduction in hours would not result in any reduced quality of care for patients.
[residency_hours.png]
I have thus managed to increase the number of available resident-hours, ensure that each resident gets the same amount of training as before, and still radically reduce the work hours from 80 per week to 40 per week. The additional recruitment each year is never more than 6,000 new residents or 15% of the current number of residents.
It takes several years to effect this transition. This is unavoidable if we are trying to avoid massive increases in recruitment, though if we were prepared to simply double the number of admitted residents each year we could immediately transition to 40-hour work weeks in a single cohort and the available resident-hours would then strictly increase every year.
This plan is likely not the optimal one; I don’t know enough about the details of how costly it would be to admit more residents, and it’s possible that some residents might actually prefer a briefer, more intense residency rather than a longer, less stressful one. (Though it’s worth noting that most people greatly underestimate the harms of stress and sleep deprivation, and doctors don’t seem to be any better in this regard.)
But this plan does prove one thing: There are solutions to this problem. It can be done. If our medical system isn’t solving this problem, it is not because solutions do not exist—it is because they are choosing not to take them.

Provocative! It would be interesting to have responses from (A) current residents, (B) those who now supervise residents, and (C) Hospital administrators.
LikeLike